Myopia is a refractive condition in which parallel rays from an object at infinity are focused in front of the retina with accommodation relaxed [1]. It is estimated that by the year 2050, 54% of the world’s population will be myopic and 10% of the world’s population will have high myopia [2]. In Nigeria, Africa’s most populous country, the prevalence of myopia in school aged children ranges between 2.7% [3] to 2.9% [4]; in adult Nigerian population the prevalence of myopia is estimated to be about 9.4% and the prevalence of high myopia is 0.7% [5]. In other African countries the prevalence of myopia varies from 1.7% in neighboring Ghana to 4.0% in South Africa [3]. The prevalence of myopia has also been reported to be higher in children in urban areas [6] compared to those in rural areas [7]. This may be due to the difference in environmental factors, duration of near work and increased screen exposure of children in urban areas.
High degrees of myopia is associated with posterior staphyloma, myopic macular degeneration, tilted optic discs [8], retinal thinning and chorio-retinal atrophy [9]. Axial length >26.5mm has been linked to faster thinning of retinal nerve fiber layer an also visual field progression [10]. Considering Africans are at risk of developing primary open angle glaucoma [11] practitioners must be more proactive in managing myopia in glaucoma suspects and confirmed glaucoma cases.

Myopia has also been related to cataracts, in particular posterior subcapsular [12] and nuclear cataracts [13]. Studies also show higher incidence of retinal detachment after cataract surgery in very high myopes compared to other refractive errors [14].
The belief that low to moderate myopia is harmless has impeded the uptake of myopia control in Africa. However, an increase in myopia by 1D is associated with a 67% increased risk of developing myopic maculopathy[15].
The purpose of this article is to enlighten the eye care practitioner on the contact lens options for myopia control, their mechanism of action, and their efficacy.
Studies show that in eyes with uncorrected myopia, there is a relative peripheral hyperopic defocus in the retina periphery. This in turn drives the peripheral retina to extend backwards in an attempt to correct the relative peripheral hyperopic defocus and thus leads to increased axial elongation of the eye [16]. Hence, contact lens options which induce peripheral myopia or a positive spherical aberration will correct the relative peripheral hyperopic defocus and lead to control of myopia progression.
Center distance multifocal and defocus contact lenses:
Centre distance multifocal contact lenses provide clear central vision while providing correction of peripheral hyperopic defocus in the peripheral retina using the addition rings inherent in the lens design. The Bifocal Lenses in Near-sighted Kids 2 (BLINK) study was a randomized control trial which studied the effect of different addition powers using a soft center distance multifocal contact lens (Biofinity D, Coppervision Inc, USA) on myopia control in children between the ages of 7 to 11 years. This study found that soft center distance multifocal lenses with add power of +2.50D provided the best form of myopia control with -0.60D change in myopia and 0.42mm axial elongation over 3 years in the high add group (+2.50D) compared to -1.05D and 0.66mm in the single vision contact lens group [17].
The presentation of myopic defocus simultaneously with optical correction has also been shown to slow axial elongation[18] even in animal models.[19] The Misight daily disposable contact lens from Coopervision offers makes use of this principle to achieve its myopia control effect.[20] Over a period of 3 years, the Misight treated group had 0.73D (59%) less myopia progression and 0.32mm (52%) less axial elongation compared to the control group. While the Misight lens is not yet widely available in Africa, the Biofinity D multifocal as well as other center distance multifocal lens designs are available in the African market.
Orthokeratology:
Orthokeratology describes the process of reshaping the cornea by making use of specially designed rigid gas permeable contact lenses. Orthokeratology may be applied to the management of myopia, hyperopia, astigmatism and presbyopia, in this article, we discus orthokeratology in relation to myopia management only.
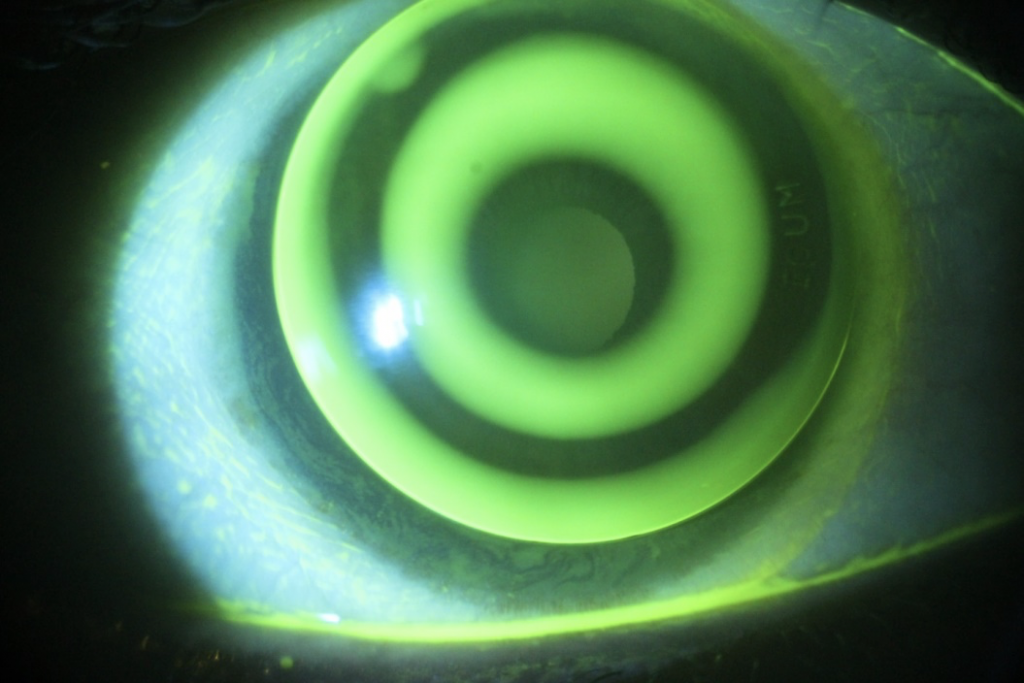
The orthokeratology lens has several zones which serve different purposes. The first zone is the treatment zone or the back optic zone radius, and it is responsible for providing the refractive change and clear vision enjoyed with the orthokeratology lens, it is usually 5mm to 6.8mm in diameter. The second zone is the reverse zone, 0.5mm to 1mm and it controls the sagittal height of the lens adding to the myopia control effect of the lens. This reverse zone creates mid-peripheral cornea steepening which creates a myopic defocus on the retina to address the peripheral hyperopic defocus and prevents myopia progression. The third zone is the lens landing zone, it is also about 0.5mm to 1mm wide and this is responsible for lens centration; it is important that the lenses do not bear heavily on the cornea to avoid epithelial erosion, but it is also important that the lenses are well centered especially on the horizontal meridian. The last zone is the edge of the lens which has a peripheral curve with a width of 0.5mm and allows for tear exchange as the lens moves over the cornea preventing lens binding and allowing for fresh oxygen to get to the cornea. These 4 zones can be appreciated once the lens sits on the cornea and its fitting relationship with the cornea is examined with sodium fluorescein dye, this is also referred to as the Bull’s eye pattern (Figure 2). Some other designs of orthokeratology incorporate more zones close to the reverse zone to address higher degrees of myopia.
The effect of the plus power created by the reverse zone corrects and addresses the peripheral hyperopic defocus which leads to myopia progression; it is recommended to make the treatment zone smaller (5.4mm). Studies show that orthokeratology lenses fit with smaller back optic zone diameter provide better myopia control compared to those with standard optic zone diameters [21]. Practitioners interested in fitting orthokeratology lenses must be trained in the science and art of the lens fitting. Excellent and reliable corneal topography testing and interpretation skills are vital for managing myopia with orthokeratology as this is important for lens designing and also troubleshooting.
Combination therapy:
While these individual strategies have proven efficacious in controlling myopia progression, there may be the need for combination therapy in some instances. Low dose atropine (0.01%) has been shown to provide a synergistic effect when used in combination with orthokeratology [22] and is currently being investigated in combination with center distance soft multifocal contact lenses [23].
Though African eye care practitioners (ECPs) are yet to see a strong statement regarding myopia control from the leading associations; practitioners must embrace myopia management as well as the contact lens options available. We must proactively offer contact lens options where indicated to our patients.
Considering the number of strategies available at the disposal of ECPs in Africa, myopia management should be embraced in clinical practice so as to serve the population requiring such services. There is also the need for further research in the field of myopia; the efficacy of the strategies and the associated complications is required in Africans.
REFERENCES
1. Goss DA, Grosvenor TP, Jeffrey OD, Keller T, Wendy Marsh-Tootle MPH, Thomas OD, et al. OPTOMETRIC CLINICAL PRACTICE GUIDELINE CARE OF THE PATIENT WITH MYOPIA Reference Guide for Clinicians Prepared by the American Optometric Association Consensus Panel on Care of the Patient with Myopia: Reviewed by the AOA Clinical Guidelines Coordinating . 2006.
2. Holden BA, Fricke TR, Wilson DA, Jong M, Naidoo KS, Sankaridurg P, et al. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 2016;123(5):1036–42.
3. Atowa UC, Munsamy AJ, Wajuihian SO. Prevalence and risk factors for myopia among school children in Aba, Nigeria. African Vis Eye Heal 2017;76(1):1–5.
4. Balarabe A, Adamu I, Abubakar A. Vision screening to detect refractive errors in three selected secondary schools in Birnin Kebbi, North West, Nigeria. Sahel Med J 2015;18(2):61.
5. Ezelum C, Razavi H, Sivasubramaniam S, Gilbert CE, Murthy GVS, Entekume G, et al. Refractive error in nigerian adults: Prevalence, type, and spectacle coverage. Investig Ophthalmol Vis Sci 2011;52(8):5449–56.
6. He M, Zeng J, Liu Y, Xu J, Pokharel GP, Ellwein LB. Refractive error and visual impairment in urban children in southern China. Investig Ophthalmol Vis Sci 2004;45(3):793–9.
7. Zhao J, Pan X, Sui R, Munoz SR, Sperduto RD, Ellwein LB. Refractive error study in children: Results from Shunyi District, China. Am J Ophthalmol 2000;129(4):427–35.
8. Chang L, Pan C-W, Ohno-Matsui K, Lin X, Cheung GCM, Gazzard G, et al. Myopia-related fundus changes in Singapore adults with high myopia. Am J Ophthalmol 2013;155(6):991-999.e1.
9. Lam DSC, King SL, Mohamed S, Chan WM, Palanivelu MS, Cheung CYL, et al. Regional variations in the relationship between macular thickness measurements and myopia. Investig Ophthalmol Vis Sci 2007;48(1):376–82.
10. S B, P B. Longitudinal Evaluation of the Structural and Functional Changes Associated with Glaucoma in Myopia. Optom Vis Sci 2020;97(6):448–56.
11. Kyari F, Abdull MM, Bastawrous A, Gilbert CE, Faal H. Epidemiology of Glaucoma in Sub-Saharan Africa: Prevalence, Incidence and Risk Factors. Middle East Afr J Ophthalmol 2013;20(2):111.
12. Younan C, Mitchell P, Cumming RG, Rochtchina E, Wang JJ. Myopia and incident cataract and cataract surgery: The blue mountains eye study. Investig Ophthalmol Vis Sci 2002;43(12):3625–32.
13. Kubo E, Kumamoto Y, Tsuzuki S, Akagi Y. Axial Length, Myopia, and the Severity of Lens Opacity at the Time of Cataract Surgery. Arch Ophthalmol 2006;124(11):1586–90.
14. G R, C S, V P, D G, DJ D, M S. Cataract surgery as a risk factor for retinal detachment in very highly myopic eyes. Ophthalmology 2003;110(12):2355–61.
15. Bullimore MA, Brennan NA. Myopia Control: Why Each Diopter Matters. Optom Vis Sci 2019;96(6):463–5.
16. Berntsen DA, Barr CD, Mutti DO, Zadnik K. Peripheral defocus and myopia progression in myopic children randomly assigned to wear single vision and progressive addition lenses. Investig Ophthalmol Vis Sci 2013;54(8):5761–70.
17. Walline JJ, Walker MK, Mutti DO, Jones-Jordan LA, Sinnott LT, Giannoni AG, et al. Effect of high add power, medium add power, or single-vision contact lenses on myopia progression in children: The BLINK randomized clinical trial. JAMA – J Am Med Assoc 2020;324(6):571–80.
18. Y L, C W. The effective add inherent in 2-zone negative lenses inhibits eye growth in myopic young chicks. Invest Ophthalmol Vis Sci 2012;53(8):5085–93.
19. B A, LF H, CH T, B H, EL S. The effects of simultaneous dual focus lenses on refractive development in infant monkeys. Invest Ophthalmol Vis Sci 2014;55(11):7423–32.
20. Chamberlain P, Peixoto-De-Matos SC, Logan NS, Ngo C, Jones D, Young G. A 3-year Randomized Clinical Trial of MiSight Lenses for Myopia Control. Optom Vis Sci 2019;96(8):556–67.
21. Loertscher M, Backhouse S, Phillips JR. Multifocal Orthokeratology versus Conventional Orthokeratology for Myopia Control: A Paired-Eye Study. J Clin Med 2021;10(3):447.
22. Sánchez-González J-M, De-Hita-Cantalejo C, Baustita-Llamas M-J, Sánchez-González MC, Capote-Puente R. The Combined Effect of Low-dose Atropine with Orthokeratology in Pediatric Myopia Control: Review of the Current Treatment Status for Myopia. J Clin Med 2020;9(8):1–13.
23. Huang J, Mutti DO, Jones-Jordan LA, Walline JJ. Bifocal & Atropine in Myopia (BAM) Study: Baseline Data andMethods. Optom Vis Sci 2019;96(5):335.